SPECIAL ISSUE: Country Responses to the COVID-19 Pandemic Articles analyzing country responses in Australia, New Zealand, Canada, U.S., Belgium, Netherlands, Sweden, France, Italy
Localisation and local humanitarian action by HPN October 2020
The theme of this edition of Humanitarian Exchange is localisation+ and local humanitarian action. Five years ago this week, donors, United Nations (UN) agencies, non-governmental organisations (NGOs), the International Committee of the Red Cross (ICRC) and International Federation of Red Cross and Red Crescent Societies (IFRC) committed within the Grand Bargain to increase multi-year investments in the institutional capacities of local and national responders, and to provide at least 25% of humanitarian funding to them as directly as possible. Since then, there is increasing consensus at policy and normative level, underscored by the Covid-19 pandemic, that local leadership should be supported. Localisation has gone from a fringe conversation among policy-makers and aid agencies in 2016 to a formal priority under the Grand Bargain. Wider global movements on anti-racism and decolonisation have also brought new momentum to critical reflections on where power, knowledge and capacity reside in the humanitarian system. Yet progress has been slow and major gaps remain between the rhetoric around humanitarian partnerships, funding and coordination and practices on the ground.
Research Letter US State-Level Legal Interventions Related to COVID-19 Vaccine Mandates
Breanna Fernandes; Mark Christopher Navin, PhD; Dorit Rubinstein Reiss, PhD; et al.
free access has active quiz
JAMA. 2022;327(2):178-179. doi:10.1001/jama.2021.22122
This study assesses state-level legal interventions to promote or impede COVID-19 vaccine mandates in the US since the beginning of the pandemic.
Antibody Response and Variant Cross-Neutralization After SARS-CoV-2 Breakthrough Infection
Timothy A. Bates, BSc; Savannah K. McBride, BSc; Bradie Winders, CNA; et al.
free access has active quiz
JAMA. 2022;327(2):179-181. doi:10.1001/jama.2021.22898
This study of fully vaccinated health care workers examines antibody levels and variant cross-neutralization after COVID-19 breakthrough infection.
Viewpoint One Year of COVID-19 Vaccines A Shot of Hope, a Dose of Reality
Amanda C. Cohn, MD; Barbara E. Mahon, MD, MPH; Rochelle P. Walensky, MD, MPH
free access has multimedia has audio
JAMA. 2022;327(2):119-120. doi:10.1001/jama.2021.23962
This Viewpoint from the CDC reviews how available vaccines have shaped the past year of the COVID-19 pandemic and the challenges that remain.
Assessment of COVID-19 vaccines acceptance in the Lebanese population: a national cross-sectional study Vaccines have become the best weapon for epidemic prevention and control in the absence of standard approved effective therapies. However, skepticism about the vaccine efficacy and safety is constantly reported. To our knowledge, there has been no study assessing COVID-19 vaccine acceptance in Lebanon. The primary objective of this survey is to assess the COVID-19 vaccines’ acceptance and its related determinants in the Lebanese population
Authors: Philippe Hanna, Aline Issa, Ziad Noujeim, Mira Hleyhel and Nadine Saleh
Content type: Research
11 January 2022
Research articles Optimal strategies to protect a sub-population at risk due to an established epidemic Elliott H. Bussell and Nik J. Cunniffe
Published:12 January 2022Article ID:20210718 https://doi.org/10.1098/rsif.2021.0718 Abstract
Epidemics can particularly threaten certain sub-populations. For example, for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the elderly are often preferentially protected. For diseases of plants and animals, certain sub-populations can drive mitigation because they are intrinsically more valuable for ecological, economic, socio-cultural or political reasons. Here, we use optimal control theory to identify strategies to optimally protect a ‘high-value’ sub-population when there is a limited budget and epidemiological uncertainty. We use protection of the Redwood National Park in California in the face of the large ongoing state-wide epidemic of sudden oak death (caused by Phytophthora ramorum) as a case study. We concentrate on whether control should be focused entirely within the National Park itself, or whether treatment of the growing epidemic in the surrounding ‘buffer region’ can instead be more profitable. We find that, depending on rates of infection and the size of the ongoing epidemic, focusing control on the high-value region is often optimal. However, priority should sometimes switch from the buffer region to the high-value region only as the local outbreak grows. We characterize how the timing of any switch depends on epidemiological and logistic parameters, and test robustness to systematic misspecification of these factors due to imperfect prior knowledge.
SARS-CoV-2 Infection in Human ACE2 Knock-In Mice
Mouse models of SARS-CoV-2 pathogenesis have facilitated the rapid evaluation of antibody and vaccine countermeasures. While the first generation of models developed severe disease after SARS-CoV-2 infection, they relied on ectopic expression of supraphysiological levels of human ACE2 (hACE2). Winkler et al. (e01511-21) evaluated SARS-CoV-2 infection in hACE2 knock-in (KI) mice, which express hACE2 under an endogenous promoter in place of murine ACE2. Infection of hACE2 KI mice with historical or variant SARS-CoV-2 strains resulted in replication within the respiratory tract but did not cause severe pulmonary injury. Thus, the hACE2 KI mouse can serve as a model of mild SARS-CoV-2 lung infection
From a pandemic perspective, 2022 seemed poised to begin with a hefty dose of déjà vu, with COVID-19 cases on the rise in many countries in the lead-up to the new year. Meanwhile, a new coronavirus variant seemed poised to overwhelm health-care systems amid fears that vaccines — from first inoculations to boosters, depending on the country — could not be rolled out quickly enough to stem the impending tsunami of infections.
The welcome news that surges of the Omicron variant are associated with less severe disease in adults than are preceding variants of SARS-CoV-2 suggests that some of pandemic modellers’ worst-case scenarios will not come to pass. But life has again been disrupted. Widespread absences due to coronavirus infections have left hospitals in many countries understaffed, forced schoolchildren to return to remote learning, and limited global mobility. And even if a relatively small percentage of those infected require hospitalization, sky-high infection rates across large populations mean that many people will still face life-threatening disease and long-term disability. This is particularly true for the unvaccinated — a group that includes a large proportion of the world’s population, especially children.
For those who had hoped that 2021 would be the year that put the pandemic in the past tense, it was a harsh reminder that it is still very much present. Rather than laying plans to return to the ‘normal’ life we knew before the pandemic, 2022 is the year the world must come to terms with the fact that SARS-CoV-2 is here to stay.
Countries must decide how they will live with COVID-19 — and living with COVID-19 does not mean ignoring it. Each region must work out how to balance the deaths, disability and disruption caused by the virus with the financial and societal costs of measures used to try to control the virus, such as mask mandates and business closures. This balance will vary from one place to another, and with time, as more therapies and vaccines become available — and as new variants emerge.
The emergence of the Omicron variant last November highlighted the ongoing challenges of life with SARS-CoV-2. Some countries were already facing surges in the highly transmissible Delta variant, but vaccines and prior infection conferred relatively high levels of protection against Delta, particularly against severe disease. Many researchers — and a fair few politicians — hoped that future waves would be less disruptive, thanks to the build-up of immunity in populations that would keep viral circulation in check and protect most people from the severe manifestations of disease that drain health-care resources.
It was expected that mutations in the viral genome would slowly chip away at this immunity, particularly its ability to stop viral transmission. But Omicron dealt a swifter and more serious blow to immunity than predicted. It is now clear that SARS-CoV-2 reinfections are more common, and that some of the most widely used COVID-19 vaccines have faltered in the face of the variant. Existing vaccines, developed against an earlier variant, now require a booster to provide substantial levels of protection against infection.
But the news has not all been grim. Vaccines, particularly when boosted, still seem to provide substantial protection against severe disease and death. Early data from animal studies suggest that Omicron might generate a different pathology compared with previous variants, causing greater infection of the upper respiratory tract and less infection in the lungs. Data from several countries suggest that the variant is associated with less severe disease, although whether this is due to the variant itself or widespread pre-existing immunity requires further study.
Countries have charted a variety of courses through the latest surge. Many with the resources have accelerated the distribution of vaccine boosters, but many others do not have this luxury. Some countries have reinstituted lockdowns, whereas others are holding back, waiting to see the extent to which climbing infection rates affect hospitals.
With infection rates soaring around the globe and many countries still unable to access adequate vaccine supplies, more SARS-CoV-2 variants of concern will continue to emerge. And, as Omicron has illustrated, the ability to predict what course those variants will take becomes more difficult as the complexities of viral evolution and pre-existing immunity complicate the models that have previously been used to anticipate the course of the pandemic. Now modellers need to factor in the effects of vaccines, previous infections, waning immunity over time, booster shots and viral variants — and, as the year progresses, they will also have to consider the impact of emerging antiviral treatments.
But what is clear is that the hope that vaccines and prior infection could generate herd immunity to COVID-19 — an unlikely possibility from the start — has all but disappeared. It is widely thought that SARS-CoV-2 will become endemic rather than extinct, with vaccines providing protection from severe disease and death, but not eradicating the virus.
As Omicron and other variants have shown, this only adds to the urgency with which vaccines must be distributed to countries that currently lack supplies. Efforts are under way to bolster vaccine production in countries such as South Africa, which have not historically been centres for vaccine manufacturing. These and other efforts to boost global access to vaccines remain in the best interests of all countries: devastating variants are particularly likely to emerge and seed blazing outbreaks in regions with low vaccination rates, and their spread will be further exacerbated where levels of testing and genomic surveillance are also low.
Fortunately, 2022 is poised to add to our defences against the pandemic. New vaccines — such as protein-based vaccines, which might cost less and have less-stringent storage requirements than mRNA vaccines currently do — will become more widely available. In December, the World Health Organization approved the long-awaited protein vaccine made by Novavax in Gaithersburg, Maryland, for emergency use. Ongoing clinical trials will establish whether upcoming vaccine candidates that target specific coronavirus variants, or that can be inhaled or taken orally rather than injected, will also be useful. Several nasal candidates are in clinical testing, including one from CanSino in Tianjin, China, and another developed by AstraZeneca in Cambridge, UK.
Meanwhile, new antiviral drugs, formulated in tablets that can be easily administered early in the course of infection to reduce the chance of serious disease and death, offer another approach against COVID-19. In the past few months, some countries have authorized the use of two such drugs: molnupiravir, made by Merck in Kenilworth, New Jersey, and Ridgeback Biotherapeutics in Miami, Florida; and Paxlovid, made by Pfizer, based in New York. Data from pivotal clinical trials of other candidates are expected in the coming year.
All of these will expand the world’s capacity to manage SARS-CoV-2 outbreaks. They are cause for hope and optimism, but with a hefty dose of realism: the virus will continue to circulate and change, and governments must continue to rely on the guidance and advice of scientists. We will not always be able to predict the virus’s path, and we must be ready to adapt with it.
Comment Unblock research bottlenecks with non-profit start-ups ‘Focused research organizations’ can take on mid-scale projects that don’t get tackled by academia, venture capitalists or government labs.
Adam Marblestone, Anastasia Gamick, Samuel G. Rodriques
It takes more than a great idea to accomplish a great project. Our research and experience have convinced us that many worthy projects wither or are never launched because neither academic laboratories, start-up firms nor government facilities can support them.
This applies particularly to projects that would produce public goods, such as data sets or tools, that could make research faster and easier. Few research-enabling projects will be commercially viable enough to attract venture capital. Nor is academia a suitable incubator. Academics can rarely muster the time, focus and workforce coordination needed to turn a proof-of-principle technology into a robust, scalable technique or to transform a research project into a platform. These engineering improvements do not fulfil teaching requirements or provide the papers or pizzazz that both senior academics and their trainees need to propel their careers.
A type of non-profit start-up could be a better way to support projects that enable research. These would have full-time scientists, engineers and executives, and total funding of about US$20 million to $100 million that would last around 5 years — longer than most grants or venture-capital funding rounds allow. And they would be set up to pursue predefined milestones, such as improving the resolution of a measurement system by tenfold, or gathering a pre-specified amount of data. We call them focused research organizations (FROs)…
Perspective Adolescents, Parents, and Covid-19 Vaccination — Who Should Decide? S. McGrew and H.A. Taylor
Covid-19 vaccination for adolescents (for these purposes, children 12 to 17 years of age) is
important, both for their own mental and physical health and for public health…
Political rationale, aims, and outcomes of health-related high-level meetings and special sessions at the UN General Assembly: A policy research observational study
Paolo Rodi, Werner Obermeyer, Ariel Pablos-Mendez, Andrea Gori, Mario C. Raviglione
Research Article | published 13 Jan 2022 PLOS Medicine https://doi.org/10.1371/journal.pmed.1003873
Recognising the substantial political weight of the United Nations General Assembly (UNGA), a UN General Assembly special session (UNGASS) and high-level meetings (HLMs) have been pursued and held for 5 health-related topics thus far. They have focused on human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS, 2001), non-communicable diseases (NCDs, 2011), antimicrobial resistance (AMR, 2016), tuberculosis (TB, 2018), and universal health coverage (UHC, 2019). This observational study presents a comprehensive analysis of the political and policy background that prompted the events, as well as an assessment of aims, approaches, and ultimate outcomes.
Effects of vaccination and non-pharmaceutical interventions and their lag times on the COVID-19 pandemic: Comparison of eight countries
Hao Li, Luqi Wang, Mengxi Zhang, Yihan Lu, Weibing Wang
Research Article | published 13 Jan 2022 PLOS Neglected Tropical Diseases https://doi.org/10.1371/journal.pntd.0010101 Abstract
Many countries implemented measures to control the COVID-19 pandemic, but the effects of these measures have varied greatly. We evaluated the effects of different policies, the prevalence of dominant variants (e.g., Delta), and vaccination on the characteristics of the COVID-19 pandemic in eight countries. We quantified the lag times of different non-pharmaceutical interventions (NPIs) and vaccination using a distributed lag non-linear model (DLNM). We also tested whether these lag times were reasonable by analyzing changes in daily cases and the effective reproductive number (Rt)over time. Our results indicated that the response to vaccination in countries with continuous vaccination programs lagged by at least 40 days, and the lag time for a response to NPIs was at least 14 days. A rebound was most likely to occur during the 40 days after the first vaccine dose. We also found that the combination of school closure, workplace closure, restrictions on mass gatherings, and stay-at-home requirements were successful in containing the pandemic. Our results thus demonstrated that vaccination was effective, although some regions were adversely affected by new variants and low vaccination coverage. Importantly, relaxation of NPIs soon after implementation of a vaccination program may lead to a rebound.
PNAS – Proceedings of the National Academy of Sciences of the United States December 21, 2021; vol. 118 no. 51 https://www.pnas.org/content/118/51
An open repository of real-time COVID-19 indicators
Alex Reinhart, Logan Brooks, Maria Jahja, Aaron Rumack, Jingjing Tang, Sumit Agrawal, Wael Al Saeed, Taylor Arnold, Amartya Basu, Jacob Bien, Ángel A. Cabrera, Andrew Chin, Eu Jing Chua, Brian Clark, Sarah Colquhoun, Nat DeFries, David C. Farrow, Jodi Forlizzi, Jed Grabman, Samuel Gratzl, Alden Green, George Haff, Robin Han, Kate Harwood, Addison J. Hu, Raphael Hyde, Sangwon Hyun, Ananya Joshi, Jimi Kim, Andrew Kuznetsov, Wichada La Motte-Kerr, Yeon Jin Lee, Kenneth Lee, Zachary C. Lipton, Michael X. Liu, Lester Mackey, Kathryn Mazaitis, Daniel J. McDonald, Phillip McGuinness, Balasubramanian Narasimhan, Michael P. O’Brien, Natalia L. Oliveira, Pratik Patil, Adam Perer, Collin A. Politsch, Samyak Rajanala, Dawn Rucker, Chris Scott, Nigam H. Shah, Vishnu Shankar, James Sharpnack, Dmitry Shemetov, Noah Simon, Benjamin Y. Smith, Vishakha Srivastava, Shuyi Tan, Robert Tibshirani, Elena Tuzhilina, Ana Karina Van Nortwick, Valérie Ventura, Larry Wasserman, Benjamin Weaver, Jeremy C. Weiss, Spencer Whitman, Kristin Williams, Roni Rosenfeld, and Ryan J. Tibshirani
PNAS December 21, 2021 118 (51) e2111452118; https://doi.org/10.1073/pnas.2111452118
Open Access
Editorial Lessons learned from leading NIH
BY Francis S. Collins
06 Jan 2022: 123-123
Having just stepped down from serving three presidents over 12 years as director of the US National Institutes of Health (NIH), I am deeply grateful for the opportunity to have led this noble enterprise and to work with amazing people. Astounding progress has been made on many fronts, including advances that I never dreamed that I would see in my lifetime—let alone during my time as NIH director…
Automation of literature screening using machine learning in medical evidence synthesis: a diagnostic test accuracy systematic review protocol Systematic review is an indispensable tool for optimal evidence collection and evaluation in evidence-based medicine. However, the explosive increase of the original literatures makes it difficult to accomplis…
Authors: Yuelun Zhang, Siyu Liang, Yunying Feng, Qing Wang, Feng Sun, Shi Chen, Yiying Yang, Xin He, Huijuan Zhu and Hui Pan
Citation: Systematic Reviews 2022 11:11
Content type: Protocol
Published on: 15 January 2022
medRxiv https://www.medrxiv.org/content/about-medrxiv medRxiv is a free online archive and distribution server for complete but unpublished manuscripts (preprints) in the medical, clinical, and related health sciences. Preprints are preliminary reports of work that have not been certified by peer review. They should not be relied on to guide clinical practice or health-related behavior and should not be reported in news media as established information. medRxiv is for the distribution of preprints – complete but unpublished manuscripts – that describe human health research conducted, analyzed, and interpreted according to scientific principles…
[Monitoring/selection from medRxiv will resume in our next edition]
Wellcome Open Research provides all Wellcome researchers with a place to rapidly publish any results they think are worth sharing. All articles benefit from rapid publication, transparent peer review and editorial guidance on making all source data openly available.
Review metrics AWAITING PEER REVIEW ‘Working relationships’ across difference – a realist review of community engagement with malaria research[version 1; peer review: awaiting peer review]
Robin Vincent, Bipin Adhikari, Claire Duddy, Emma Richardson, Geoff Wong, James Lavery, Sassy Molyneux, The REAL team: Mary Chambers, Phaik Yeong Cheah, Al Davies, Kate Gooding, Dorcas Kamuya, Vicki Marsh, Noni Mumba, Deborah Nyirenda, and Paulina Tindana.
Peer Reviewers Invited
Funders
Wellcome
Human Engagement Learning Platform (Bill and Melinda Gates Foundation)
Emory University
PUBLISHED 13 Jan 2022
Kaiser Family Foundation https://www.kff.org/search/?post_type=press-release Accessed 15 Jan 2022
[No new digest content identified] Rand [to 15 Jan 2022] https://www.rand.org/pubs.html Reports, Selected Journal Articles Research Brief Early Insights from the Equity-First Vaccination Initiative
The Equity-First Vaccination Initiative aims to reduce racial/ethnic disparities in COVID-19 vaccination rates in the United States. Five demonstration sites are using hyper-local, community-led strategies to increase vaccine confidence and access.
Dec 20, 2021
Laura J. Faherty, Jeanne S. Ringel, Malcolm V. Williams, Ashley M. Kranz, Lilian Perez, Lucy Schulson, Allyson D. Gittens, Brian Phillips, Lawrence Baker, Priya Gandhi, Khadesia Howell, Rebecca Wolfe, Tiwaladeoluwa
Vaccines and Global Health: The Week in Review is a weekly digest summarizing news, events, announcements, peer-reviewed articles and research in the global vaccine ethics and policy space. Content is aggregated from key governmental, NGO, international organization and industry sources, key peer-reviewed journals, and other media channels. This summary proceeds from the broad base of themes and issues monitored by the Center for Vaccine Ethics & Policy in its work: it is not intended to be exhaustive in its coverage. You are viewing the blog version of our weekly digest, typically comprised of between 30 and 40 posts below all dated with the current issue date
.– Request anEmail Summary:Vaccines and Global Health : The Week in Review is published as a single email summary, scheduled for release each Saturday evening before midnight (EDT in the U.S.). If you would like to receive the email version, please send your request to david.r.curry@centerforvaccineethicsandpolicy.org.
– pdf version: A pdf of the current issue is available here:
– blog edition: comprised of the approx. 35+ entries posted below.
– Twitter:Readers can also follow developments on twitter: @vaxethicspolicy. . – Links: We endeavor to test each link as we incorporate it into any post, but recognize that some links may become “stale” as publications and websites reorganize content over time. We apologize in advance for any links that may not be operative. We believe the contextual information in a given post should allow retrieval, but please contact us as above for assistance if necessary.
Support this knowledge-sharing service:Your financial support helps us cover our costs and to address a current shortfall in our annual operating budget. Click here to donate and thank you in advance for your contribution.
. David R. Curry, MS Executive Director Center for Vaccine Ethics and Policy
I hope global leaders who have shown such resolve in protecting their own populations will extend that resolve to make sure that the whole world is safe and protected. And this pandemic will not end until we do that!
Last week, I asked everyone to make a New Year’s resolution to get behind the campaign to vaccinate 70% of people in every country by the middle of 2022. And on top of that, to ensure that breakthrough treatments, as well as reliable tests, are available in all countries. To end the acute stage of the pandemic, the highly effective tools science has given us need to be shared fairly and quickly with all countries of the world.
Vaccine inequity and health inequity overall were the biggest failures of last year. While some countries have had enough personal protective equipment, tests and vaccines to stockpile throughout this pandemic, many countries do not have enough to meet basic baseline needs or modest targets, which no rich country would have been satisfied with.
Vaccine inequity is a killer of people and jobs and it undermines a global economic recovery. Alpha, Beta, Delta, Gamma and Omicron reflect that in part because of low vaccination rates, we’ve created the perfect conditions for the emergence of virus variants. Last week, the highest number of COVID-19 cases were reported so far in the pandemic.
And we know, for certain, that this is an underestimate of cases because reported numbers do not reflect the backlog of testing around the holidays, the number of positive self-tests not registered, and burdened surveillance systems that miss cases around the word. While Omicron does appear to be less severe compared to Delta, especially in those vaccinated, it does not mean it should be categorized as ‘mild’. Just like previous variants; Omicron is hospitalizing people and it is killing people. In fact, the tsunami of cases is so huge and quick, that it is overwhelming health systems around the world.
Hospitals are becoming overcrowded and understaffed, which further results in preventable deaths from not only COVID-19 but other diseases and injuries where patients cannot receive timely care.
First-generation vaccines may not stop all infections and transmission but they remain highly effective in reducing hospitalization and death from this virus.
So as well as vaccination, public health social measures, including the wearing of well fitting masks, distancing, avoiding crowds and improving and investing in ventilation are important for limiting transmission. At the current pace of vaccine rollout, 109 countries would miss out on fully vaccinating 70% of their populations by the start of July 2022.
The essence of the disparity is that some countries are moving toward vaccinating citizens a fourth time, while others haven’t even had enough regular supply to vaccinate their health workers and those at most risk. Booster after booster in a small number of countries will not end a pandemic while billions remain completely unprotected. But we can and must turn it around. In the short-term we can end the acute stage of this pandemic while preparing now for future ones.
First, we must effectively share the vaccines that are being produced.
Throughout most of 2021 this was not the case but toward the end, supply increased. Now it’s crucial that manufacturers and dose-donating countries share delivery timings ahead of time so that countries have adequate preparation to roll them out effectively.
Second, let’s take a ‘never again’ approach to pandemic preparedness and vaccine manufacturing so that as soon as the next generation of COVID-19 vaccines become available, they are produced equitably and countries don’t have to beg for scarce resources. A few countries have provided a blueprint for how high quality vaccines and other health tools can be mass produced quickly and distributed effectively. And now we need to build on it. WHO will continue to invest in vaccine manufacturing hubs and work with any and all manufacturers who are willing to share know-how, technology and licenses. I’m encouraged by some of the vaccines currently going through trial where innovators have already committed to waiving patents and sharing licenses, technology and know how.
It reminds me of how Jonas Salk did not patent his polio vaccine and in doing so saved millions of children from the disease.
Lets also invest and build the public health and health systems we need with strong surveillance, adequate testing, a strengthened, supported and protected health workforce, and an empowered, engaged and enabled global population.
And finally, I call on citizens of the world, including civil society, scientists, business leaders, economists and teachers to demand that governments and pharmaceutical companies to share health tools globally and bring an end to the death and destruction of this pandemic.
We need vaccine equity, treatment equity, test equity and health equity and we need your voices to drive that change.
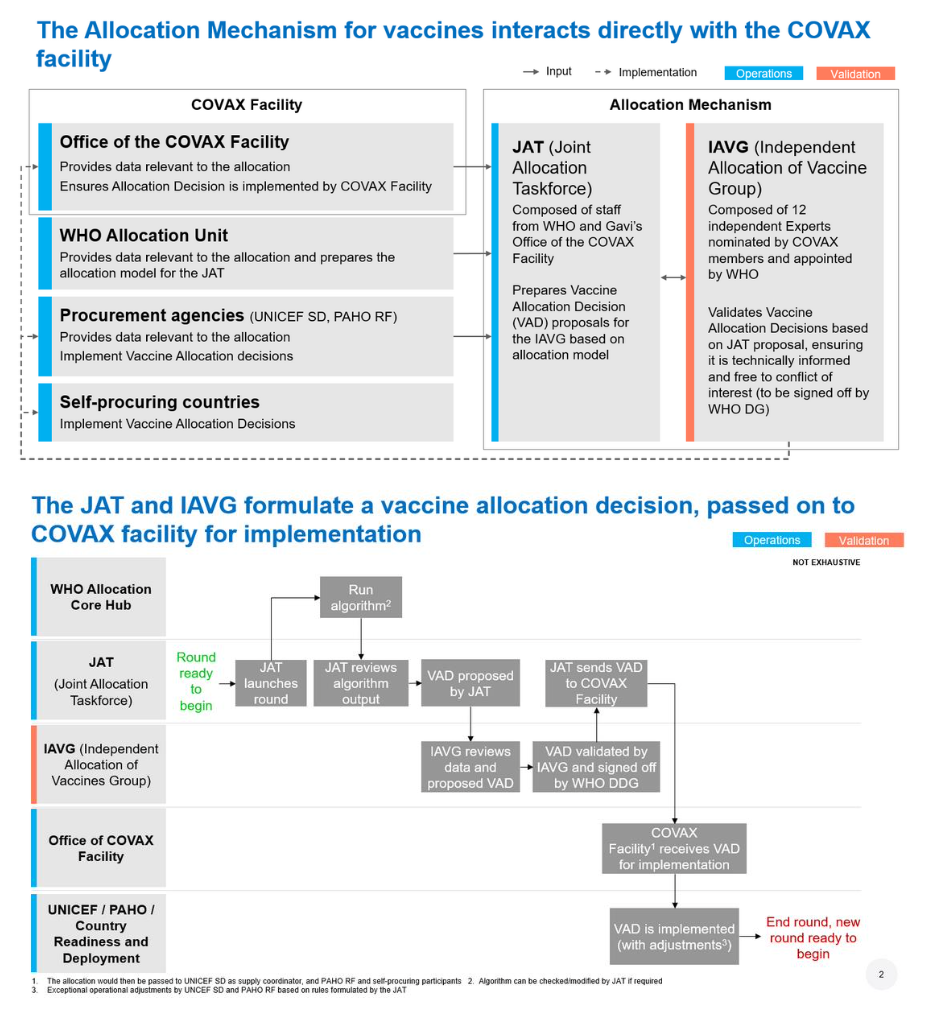
Achieving 70% COVID-19 Immunization Coverage by Mid-2022 Statement of the Independent Allocation of Vaccines Group (IAVG) of COVAX 23 December 2021 The Independent Allocation of Vaccines Group (IAVG) has issued a set of recommendations to make the allocation of COVID-19 vaccines more equitable and more effective. The group was established a year ago, to validate and assess vaccine allocations recommended by WHO’s and Gavi’s Joint Allocation Taskforce (JAT) of COVAX. [1] Since then, much has changed.
COVAX was envisioned to be the world’s primary distributor of COVID-19 vaccines, with IAVG serving as an independent referee for needs-based allocations. But rich nations largely sidestepped COVAX, hoarding doses for their own populations and cutting deals directly with low- and middle-income countries. This has made subsequent allocation decisions even more challenging.
The IAVG is concerned that the primary priority use of available vaccines is not consistent with the goals outlined in the Strategy to Achieve Global COVID-19 Vaccination by Mid-2022 in October 2021. [2] The group also notes that it has validated the allocation of only 730 million of the estimated 8 billion doses of vaccine that have been administered globally, which is less than 10%. The rapid emergence of the Omicron variant is a stark reminder of the ongoing threat posed by the evolution of the COVID-19 pandemic and reinforces the critical need to achieve high levels of immunization coverage in all countries, including in highly vulnerable populations, in a timely manner.
The IAVG is therefore calling for: :: Achievement of 70% coverage with COVID-19 vaccines in all countries as a global imperative. As the overall vaccine supply to COVAX is anticipated to continue to grow substantially next year, COVAX will have a greater opportunity to contribute to achieving this goal. Manufacturers, vaccine-producing and high-coverage countries must prioritize vaccine equity and transparency, including the sharing of information about manufacturing capacity and supply schedules with COVAX, as well as vaccine access plans.
:: All countries to work with COVAX with considerable urgency to optimize the strategic use of the growing vaccine supply. This means that high-coverage countries will need to establish complementary, “dual-track” approaches that consider both domestic and international goals. Greater attention must be paid to who is being immunized. Equity must remain the overarching principle, and priority must be given in all countries to ensuring that the primary series is offered first and foremost to all adults and adolescents, in the step-wise manner recommended by the WHO, given that a high proportion of these populations still require primary immunization. However, as more is known about the required vaccination response in the face of Omicron, the need for booster doses and need to immunize children, the COVAX vaccine allocation decisions must consider these recommendations. Given the global health and epidemiologic consequences of failing to immunize vulnerable populations, including those in humanitarian settings, the IAVG recommends that COVAX continue to work with all manufacturers and countries to immediately increase the availability and uptake of vaccines in these populations.
:: All countries to have a steady, predictable supply of COVID-19 vaccines, which meet the unique needs of each country. Attention must be paid to addressing prohibitive absorptive challenges in countries that request support. This may include support for vaccine storage, distribution, administration and/or record-keeping, which may in part be due to competing health and immunization crises [3]. It will be important to have close collaboration between all COVAX partners, donors, and participants. In order to increase demand for COVID-19 vaccines, ongoing, concerted global, national and local leadership is required to address vaccine misinformation.
Background The initial COVAX targets were to achieve 3% coverage, and then 20% vaccine coverage through COVAX-secured doses by the end of 2021. [4] These targets were then expanded globally, when WHO released the Strategy to Achieve Global COVID-19 Vaccination by Mid-2022 in October 2021. [5] The new global target is 40% total population coverage by the end of 2021, and 70% total population coverage by mid-2022. However, these figures were from all country sources of supply, not solely from COVAX. COVAX would nonetheless contribute as much as possible to efforts to reach this coverage level in a fair and equitable manner.
None of these targets have been met. Ninety-eight countries have not vaccinated 40% of their population. An estimated 1.4 billion eligible people [6] need to be urgently immunized, many of whom are in the highest risk groups for death and serious illness. These gaps have been most pronounced in low-and lower-middle income countries (LICs and LMICs), with 34 out of 89 Advanced Market Commitment (AMC) participants,[7] representing the countries that are most dependent on COVAX to access COVID-19 vaccines, not achieving the 40% target. The main reason for this has been the severe vaccine supply constraints to COVAX, which persisted until the last quarter of 2021. In the forthcoming months, larger volumes of vaccine are expected to become available, but in most cases the increase in volumes will create challenges in absorption capacity in resource-poor settings. This includes the capacity to receive, store, distribute, administer (due, for example, the lack of trained health personnel or vaccination centers), and to record vaccine use, including wastage.
Another hurdle in achieving the target of 70% total population coverage in all countries by mid-2022 will be demand limits arising from widespread misinformation and its resulting vaccine hesitancy.
Challenges The COVAX portion of the global supply – The original goal of COVAX was to achieve fair and equitable vaccine access across all 162 current Facility participants, and the initial role of the IAVG was to validate vaccine allocation decision (VAD) proposals that included all participants. Many high-income countries (HICs) entered into direct contractual arrangements with vaccine suppliers, bypassing the COVAX mechanism, and pharmaceutical companies did not prioritize and deliver according to their contractual obligations with COVAX, seriously reducing its supply and making it highly unpredictable.
Moreover, high-coverage countries began donating directly to their low-coverage and low-income counterparts, bypassing COVAX. Indemnity and liability-related conditions are added barriers to the vaccine access for the most vulnerable populations. The IAVG has validated the allocation of only 730 million of the estimated 8 billion doses of vaccine that have been administered globally, which is less than 10%.
Additionally, many of the donated doses channeled through COVAX have been earmarked for specific countries, compounding the challenge of achieving the goal of fair and equitable access among lower income countries.
With respect to vaccine allocation, the IAVG recommended and acknowledges that, where feasible, the limited COVAX supply has recently been dedicated to those countries with low estimated total population coverage which are likely relying solely on COVAX for access to COVID-19 vaccines.
Unpredictable supply to COVAX – 1) Procured doses – While those involved in vaccine allocation through COVAX have done their best to direct and redirect available doses, supply unpredictability has strained the system, frustrated participating countries and undermined the allocation decisions of the IAVG. Not all expected doses from COVAX advanced purchase agreements (APAs) have been honoured by vaccine producers according to contractual obligations. 2) Donated volumes – Similarly, promised donations by high-income countries have often been late to materialize or unpredictable. Unexpected additional vaccine allocation rounds have been undertaken after sudden announcements of vaccine availability through donations to COVAX. Worsening the challenge, these sudden donations have often included vaccines with brief expiry windows. These last-minute scrambles, a part massively increasing transaction costs, added considerable stress to already severely resource-strapped countries coping with many competing health and humanitarian crises, straining participants’ ability to plan for the receipt and use of their allocated vaccines. Beyond logistics, the last-minute deliveries undermined countries’ efforts to inform the general public about the vaccines and the communication needed to counteract the misinformation spread by social media.
This way of doing business is not acceptable and needs to end.
Across country and in-country inequity – The Global COVID-19 Vaccination Strategy [8] clearly outlines the step-by-step process needed to achieve the immediate goal of minimizing deaths, severe disease and overall disease burden, and reducing the risk of new variants. Older adults and high-risk populations, all adults, and adolescents have been prioritized in a step-wise manner, while the broader scope of vaccine-use recommendations is still under consideration. For instance, 15 times [9] as many booster doses are currently being administered globally as are primary doses in LICs. In October, the WHO and many other concerned partners [10] noted that data from 119 countries suggest that by September 2021, two in five health and care workers (HCW) were vaccinated on average. But the differences across regions and economic groups remained stark. For instance, less than one in ten have been fully vaccinated in the African region while four in five have been vaccinated in 22 mostly high income countries.
The IAVG is concerned that the primary priority use of available vaccines is not consistent with the goals outlined the Strategy.
More supply but more unknowns – Although the world is expected to have enough COVID-19 vaccine doses by mid-2022 to vaccinate 70% of the world’s population with three doses, [11] uncertainties abound. These include the possible need for variant-specific vaccines, changes to vaccination policies, country preference for some products over others, the programmatic complexity of managing multiple products, and the need for better intelligence on country-level planning and execution.
The uncertainty of the required vaccination response to the Omicron variant will necessitate ongoing attention to achieving fairness and equity while requiring flexibility in vaccine allocation and supply management.
Highly vulnerable populations – Our collective health security depends on the health security of all populations wherever they are, and whatever status they may have in individual countries. Among them, people residing in humanitarian settings (refugees, internally displaced persons) are at considerably increased risk of infection with COVID-19 [12] and should be covered by country vaccine allocations.
Joint Statement of the Multilateral Leaders Taskforce on Scaling Covid-19 Tools, December 17, 2021: “From Vaccines to Vaccinations”
Washington, December 22, 2021 — The heads of the International Monetary Fund, World Bank Group, World Health Organization, and World Trade Organization held high-level consultations with Gavi and UNICEF on December 17, 2021 aimed at increasing the use of COVID-19 vaccines and other critical medical countermeasures in low-income (LIC) and lower middle-income (LMIC) countries and supporting countries to be better prepared, resourced, and ready to roll out vaccines.
We agreed on the urgency to accelerate vaccinations in LICs, where under 5% of the population is fully vaccinated, as well as in LMICs, where around 30% of the population is fully vaccinated. We agreed to work with countries to support and strengthen their national vaccination goals consistent with the global target to vaccinate 70% of the populations in all countries by mid-2022. The emergence of the Omicron variant underscores the vital need for fair and broad access to vaccines as well as testing, sequencing, and treatments to end the pandemic.
Addressing vaccine inequity, particularly in LICs, requires increasing the supplies of vaccines to COVAX and AVAT, encouraging LICs and LMICs to purchase additional vaccine doses, and enhancing country readiness to deploy vaccines. Furthermore, to facilitate trade flows to support the manufacturing and distribution of vaccines and other COVID tools, export restrictions must be rolled back and trade-facilitating measures must be put in place. Fully funding the ACT-A Accelerator’s Financing Framework would play an important role in narrowing these gaps and reaching the global target.
Some LICs and LMICs are facing serious challenges in vaccine deployment. Constraints related to storage, cold chain capacity, and trained vaccinators are exacerbated in some cases by doses arriving with short shelf lives and without adequate lead time and shortages in ancillary supplies (such as syringes, safety boxes, and dilutants), with challenges to plan and finance vaccination campaigns in a timely manner. As in wealthier countries, vaccine hesitancy is also an issue in some LICs and LMICs.
To address such challenges, we call on governments that have already achieved high coverage to: fulfill their donation pledges as quickly as possible to accelerate near-term deliveries to COVAX; release manufacturers from contracts and options and implement delivery swaps, so they can prioritize supply to COVAX, AVAT, and low-coverage countries.
We urge governments that have yet to achieve high vaccination coverage to: contract additional doses immediately through AVAT, COVAX, or bilaterally; establish in-country surge capacity to increase the rate of vaccine utilization as supplies increase; and coordinate between health and finance authorities for making increased use of multilateral development banks’ resources that are readily available for both vaccine purchase and deployment.
We call for better coordination among vaccine manufacturers, dose donating countries, COVAX, AVAT, and other partners to improve visibility on vaccine supply schedules and quality of supply for LICs and LMICs, to support country-level planning and preparedness for turning vaccines into vaccinations. Visibility on schedules along with adequate lead times and shelf lives of vaccines are critical for both equitable distribution as well as for recipient countries and their partners to prepare for in-country deployment.
Growing volumes of COVID-19 vaccines are forecast to arrive in LICs and LMICs in the coming months. Close coordination amongst all stakeholders will be crucial to help provide countries with the assistance and necessary resources to increase their capacity to administer those doses. In this regard, we welcome the recent appointment by UNICEF and WHO, in partnership with Gavi, of the Global Lead Coordinator for COVID Vaccine Country Readiness and Delivery, who will play an important key role in strengthening in-country vaccine deployment.
::::::
UNICEF and WHO, in partnership with Gavi, ask Ted Chaiban to serve as Global Lead Coordinator for COVID Vaccine Country Readiness and Delivery Statement by UNICEF Executive Director Henrietta Fore
NEW YORK, 6 December 2021 – “I am pleased to announce that UNICEF and WHO, in partnership with Gavi, have asked Ted Chaiban, currently UNICEF Regional Director Middle East and North Africa, to serve as Global Lead Coordinator for COVID Vaccine Country Readiness and Delivery. “This decision is an expression of our joint commitment to reinvigorate efforts to turn vaccines into vaccinations in low- and middle-income countries…