Research Letter SARS-CoV-2–Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women
Sivan Haia Perl, MD; Atara Uzan-Yulzari, MSc; Hodaya Klainer, BSc; et al.
free access has active quiz
JAMA. 2021;325(19):2013-2014. doi:10.1001/jama.2021.5782
This prospective study investigated whether antibodies from SARS-CoV-2 immunization of nursing mothers transferred to infants as a potentially protective effect.
Viewpoint Digital Health Passes in the Age of COVID-19Are “Vaccine Passports” Lawful and Ethical?
Lawrence O. Gostin, JD; I. Glenn Cohen, JD; Jana Shaw, MD, MPH
free access
JAMA. 2021;325(19):1933-1934. doi:10.1001/jama.2021.5283
This Viewpoint discusses digital health passes (DHPs) that would grant access to work, entertainment, shopping, and travel with confirmation of COVID-19 immunity, and the scientific, legal, ethical, and equity considerations that must be worked through for DHPs to be considered effective and fair.
Viewpoint Incorporating Adult Evidence Into Pediatric Research and PracticeBayesian Designs to Expedite Obtaining Child-Specific Evidence
Srinivas Murthy, MD, CM, MHSc; Patricia Fontela, MD; Scott Berry, PhD
free access
JAMA. 2021;325(19):1937-1938. doi:10.1001/jama.2020.25007
This Viewpoint proposes ways to use bayesian methods to integrate evidence from adult clinical trials into the conduct, interpretation, and application of pediatric trials to generate scientifically robust and clinically actionable data for the care of children at a pace comparable with that for adults
Editorial | 20 May 2021 The value of evidence synthesis
Science is a cumulative enterprise, and systematic evidence synthesis is invaluable for appraising what is known and what is not known on a specific research question. We strongly encourage the submission of systematic reviews and meta-analyses to Nature Human Behaviour.
Article | 30 March 2021 Socioeconomic impacts of COVID-19 in low-income countries
Recent phone survey data from Ethiopia, Malawi, Nigeria and Uganda reveals the breadth of the socioeconomic impacts of the COVID-19 pandemic on individuals and households.
Anna Josephson, Talip Kilic, Jeffrey D. Michler
Vaccine hesitancy among paediatric nurses: Prevalence and associated factors
Usue Elizondo-Alzola, Mireia G. Carrasco, Laia Pinós, Camila Andrea Picchio, Cristina Rius, Elia Diez
Research Article | published 19 May 2021 PLOS ONE https://doi.org/10.1371/journal.pone.0251735
PNAS – Proceedings of the National Academy of Sciences of the United States of America
May 11, 2021; vol. 118 no. 19 https://www.pnas.org/content/118/19
Opinion Leading scientists discuss current issues Opinion: Compound risks and complex emergencies require new approaches to preparedness
A. Kruczkiewicz, J. Klopp, J. Fisher, S. Mason, S. McClain, N. M. Sheekh, R. Moss, R. M. Parks, and C. Braneon
PNAS May 11, 2021 118 (19) e2106795118; https://doi.org/10.1073/pnas.2106795118
Increasingly, we face compounding and interrelated environmental, socioeconomic, and political crises. Yet our approaches to these problems are often siloed, fragmented, and inadequate. The current pandemic, for instance, continues to collide with a number of other threats to human life and livelihoods. These include violent conflicts, displacement, insect swarms, droughts, heat waves, and structural inequality in the form of racism and gender discrimination. We believe we are at a critical juncture, faced with a need and responsibility to redesign institutions to be proactive, agile, and socially just when confronted with increasingly likely compound risks…
Open Access Commentary COVID-19 Pandemic and Equal Access to Vaccines
by Matteo Bolcato et al
Vaccines 2021, 9(6), 538; https://doi.org/10.3390/vaccines9060538 (registering DOI) – 21 May 2021 Abstract
The COVID-19 pandemic has evidenced the chronic inequality that exists between populations and communities as regards global healthcare. Vaccination, an appropriate tool for the prevention of infection, should be guaranteed by means of proportionate interventions to defeat such inequality in populations and communities […
Media/Policy Watch
This watch section is intended to alert readers to substantive news, analysis and opinion from the general media and selected think tanks and similar organizations on vaccines, immunization, global public health and related themes. Media Watch is not intended to be exhaustive, but indicative of themes and issues CVEP is actively tracking. This section will grow from an initial base of newspapers, magazines and blog sources, and is segregated from Journal Watch above which scans the peer-reviewed journal ecology.
We acknowledge the Western/Northern bias in this initial selection of titles and invite suggestions for expanded coverage. We are conservative in our outlook in adding news sources which largely report on primary content we are already covering above. Many electronic media sources have tiered, fee-based subscription models for access. We will provide full-text where content is published without restriction, but most publications require registration and some subscription level.
The sheer volume of vaccine and pandemic-related coverage is extraordinary. We will strive to present the most substantive analysis and commentary we encounter.
Asia Pacific Pakistan’s Private Vaccine Sales Highlight Rich-Poor Divide
An inoculation push, plagued with limited supplies and red tape, makes doses available to those who can pay for them. In a country with a struggling economy, most can’t.
By Salman Masood May 22, 2021
Politics 100 Million Vaccine Doses Held Up Over Contamination Concerns, Firm Reveals
Executives from Emergent, which ruined millions of coronavirus vaccine doses, divulged to Congress the scope of the regulatory review of its troubled Baltimore plant.
By Sheryl Gay Stolberg and Sharon LaFraniere May 22, 2021
World A vaccine maker in India signals it won’t export doses before year’s end, slowing aid to the world’s poorest.
By Sameer Yasir May 19, 2021
The vaccination woes of some of the world’s poorest nations will continue as the Serum Institute of India, a crucial manufacturing pillar in the plan to supply two billion doses of Covid-19 vaccines to low-income countries, signaled that it would not be able to provide vaccines beyond India before the year’s end.
The revelation, tucked into a statement by the vaccine manufacturing giant that attempted to deflect mounting criticism, was another setback for Covax, the global vaccine partnership for the poor. It is already more than 140 million doses behind schedule, and the Serum Institute’s announcement suggested it was all but impossible to meet the goal of two billion doses by the end of the year.
The announcement once again underscored the glaring contrast of inequality: As some of the richer nations tout levels of vaccinations that allow them to reopen their society, most of the poorer nations have barely gotten a start.
“We continue to scale up manufacturing and prioritize India,” the Serum Institute of India said in the statement on Tuesday. “We also hope to start delivering to Covax and other countries by the end of this year.”…
Think Tanks et al Brookings http://www.brookings.edu/ Accessed 22 May 2021 [No new digest content] Center for Global Development [to 22 May 2021] http://www.cgdev.org/page/press-center Content Dear President Biden and Congress: Time for US to Lead Response to the Growing COVID-19 Global Vaccine Crisis
May 17, 2021
Today we joined colleagues from CSIS, Duke University, and the COVID Collective in an open letter to the Biden Administration and US Congress with a clear message: to hasten the end of the COVID-19 global pandemic, American leadership is required to ensure universal global access to high-quality and safe vaccines, support rapid vaccine distribution and administration, and build a sustainable global network of vaccine manufacturing capacity. Vaccines offer an exit route out of the pandemic – but only if they reach a critical mass of people in need across continents, socioeconomic strata, and marginalized populations. Amanda Glassman, Rachel Silverman and Prashant Yadav
Vaccines and Global Health: The Week in Review is a weekly digest summarizing news, events, announcements, peer-reviewed articles and research in the global vaccine ethics and policy space. Content is aggregated from key governmental, NGO, international organization and industry sources, key peer-reviewed journals, and other media channels. This summary proceeds from the broad base of themes and issues monitored by the Center for Vaccine Ethics & Policy in its work: it is not intended to be exhaustive in its coverage. You are viewing the blog version of our weekly digest, typically comprised of between 30 and 40 posts below all dated with the current issue date
.– Request anEmail Summary:Vaccines and Global Health : The Week in Review is published as a single email summary, scheduled for release each Saturday evening before midnight (EDT in the U.S.). If you would like to receive the email version, please send your request to david.r.curry@centerforvaccineethicsandpolicy.org.
– pdf version: A pdf of the current issue is available here:
– blog edition: comprised of the approx. 35+ entries posted below.
– Twitter:Readers can also follow developments on twitter: @vaxethicspolicy. . – Links: We endeavor to test each link as we incorporate it into any post, but recognize that some links may become “stale” as publications and websites reorganize content over time. We apologize in advance for any links that may not be operative. We believe the contextual information in a given post should allow retrieval, but please contact us as above for assistance if necessary.
Support this knowledge-sharing service:Your financial support helps us cover our costs and to address a current shortfall in our annual operating budget. Click here to donate and thank you in advance for your contribution.
. David R. Curry, MS Executive Director Center for Vaccine Ethics and Policy
COVID-19: Make it the Last Pandemic The Independent Panel for Pandemic Preparedness and Response May 2021 :: 86 pages The Independent Panel was established by the World Health Organization (WHO) Director-General in response to the World Health Assembly resolution 73.1. The mission of the Independent Panel is to provide an evidence-based path for the future, grounded in lessons of the present and the past to ensure countries and global institutions, including specifically WHO, effectively address health threats. Members: Rt Hon. Helen Clark Co-Chair H.E. Ellen Johnson Sirleaf Co-Chair Mauricio Cárdenas Aya Chebbi Mark Dybul Michel Kazatchkine Joanne Liu Precious Matsoso David Miliband Thoraya Obaid Preeti Sudan Ernesto Zedillo Zhong Nanshan
Main Report: COVID-19: Make it the Last Pandemic – PDF, 5.1 MB From the Introduction …Seized by the gravity of the crisis, in May 2020 the World Health Assembly requested the Director-general of WHO to initiate an impartial, independent, and comprehensive review of the international health response to COVID-19 and of experiences gained and lessons learned from that, and to make recommendations to improve capacities for the future. The Director-General asked H.E. Ellen Johnson Sirleaf and the Rt Hon. Helen Clark to convene an independent panel for this purpose and to report to the World Health Assembly in May 2021.
The Panel has taken a systematic, rigorous and comprehensive approach to its work. It has sought to listen to and learn from a wide range of interlocutors. Since mid-September 2020, the Panel has reviewed extensive literature, conducted original research, heard from experts in 15 round-table discussions and in interviews, received the testimony of people working on the front lines of the pandemic in town-hall-style meetings, and welcomed many submissions from its open invitation to contribute.
The Panel has examined the state of pandemic preparedness prior to COVID-19, the circumstances of the identification of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the disease it causes, coronavirus disease (COVID-19), and responses globally, regionally and nationally, particularly in the pandemic’s early months. It has also analysed the wide-ranging impact of the pandemic and the ongoing social and economic crisis that it has precipitated.
This report presents the Panel’s findings on what happened, the lessons to be learned from that, and our recommendations for strategic action now to end this pandemic and to ensure that any future infectious disease outbreak does not become a catastrophic pandemic…
[Excerpts; Editor’s selection/text bolding] [p.14] The Independent Panel makes the following urgent calls I. Apply non-pharmaceutical public health measures systematically and rigorously in every country at the scale the epidemiological situation requires. All countries to have an explicit evidence-based strategy agreed at the highest level of government to curb COVID-19 transmission.
II. High income countries with a vaccine pipeline for adequate coverage should, alongside their scale up, commit to provide to the 92 low and middle income countries of the Gavi COVAX Advance Market Commitment, at least one billion vaccine doses no later than 1 September 2021 and more than two billion doses by mid-2022, to be made available through COVAX and other coordinated mechanisms.
III. G7 countries to commit to providing 60% of the US$ 19 billion required for ACT-A in 2021 for vaccines, diagnostics, therapeutics and strengthening health systems with the remainder being mobilised from others in the G20 and other higher income countries. A formula based on ability to pay should be adopted for predictable, sustainable, and equitable financing of such global public goods on an ongoing basis.
IV. The World Trade Organization and WHO to convene major vaccine-producing countries and manufacturers to get agreement on voluntary licensing and technology transfer arrangements for COVID-19 vaccines (including through the Medicines Patent Pool). If actions do not occur within three months, a waiver of intellectual property rights under the Agreement on Trade-Related Aspects of Intellectual Property Rights should come into force immediately.
V. Production of and access to COVID-19 tests and therapeutics, including oxygen, should be scaled up urgently in low- and middle income countries with full funding of US$1.7 billion for needs in 2021 and the full utilization of the US$3.7 billion in the Global Fund’s COVID-19 Response Mechanism Phase 2 for procuring tests, strengthening laboratories and running surveillance and tests.
VI. WHO to develop immediately a roadmap for the short-term, and within three months scenarios for the medium- and long-term response to COVID-19, with clear goals, targets and milestones to guide and monitor the implementation of country and global efforts towards ending the COVID-19 pandemic.
[p.45] 5. The Independent Panel’s recommendations for transforming the international system for pandemic preparedness and response The Panel believes that system-level change is needed to overcome the manifest failure of the international system to prevent, contain, and mitigate the impact of a pandemic. Pandemic preparedness and response have to function at national, regional and global levels, across different sectors of social and economic life, and include government, business and community.
The current pandemic needs to be stopped as quickly as possible. Then measures in the recovery phase must be taken to ensure that such a pandemic never happens again, by building forward better. The lost ground in progress towards the Sustainable Development Goals needs to be made up by redressing the interlocking impacts of the pandemic on health, livelihoods, and inequality.
The Panel’s recommendations follow from the diagnosis we have made of what went wrong at each stage of the pandemic, in preparedness, surveillance and alert and early and sustained response and from our view of the leadership required to transform the system.
There is a need for: :: Stronger leadership and better coordination at national, regional and international level, including a more focused and independent WHO, a Pandemic Treaty, and a senior Global Health Threats Council. :: investment in preparedness now, and not when the next crisis hits, more accurate measurement of it, and accountability mechanisms to spur action; :: an improved system for surveillance and alert at a speed that can combat viruses like SARS-CoV-2, and authority given to WHO to publish information and to dispatch expert missions immediately; :: a pre-negotiated platform able to produce vaccines, diagnostics, therapeutics and supplies and secure their rapid and equitable delivery as essential global common goods; :: access to financial resources, both for investments in preparedness and to be able to inject funds immediately at the onset of a potential pandemic.
The Panel calls on Member States to request the United Nations Secretary-General to convene a special session of the United Nations General Assembly to reach agreement on the reforms needed to ensure that the world can prevent the next outbreak of a new pathogen becoming another pandemic…
[p.48] 2. Focus and strengthen the independence, authority and financing of the WHO The Panel recommends I. Establish WHO´s financial independence, based on fully unearmarked resources, increase Member States fees to 2/3 of the budget for the WHO base programme and have an organized replenishment process for the remainder of the budget.
II. Strengthen the authority and independence of the Director-General, including by having a single term of office of seven years with no option for re-election. The same rule should be adopted for Regional Directors.
III. Strengthen the governance capacity of the Executive Board, including by establishing a Standing Committee for Emergencies.
IV. Focus WHO’s mandate on normative, policy, and technical guidance, including supporting countries and regions to build capacity for pandemic preparedness and response and for resilient and equitable health systems.
V. Empower WHO to take a leading, convening, and coordinating role in operational aspects of an emergency response to a pandemic, without, in most circumstances, taking on responsibility for procurement and supplies, while also ensuring other key functions of WHO do not suffer including providing technical advice and support in operational settings.
VI. Resource and equip WHO Country Offices sufficiently to respond to technical requests from national governments to support pandemic preparedness and response, including support to build resilient equitable and accessible health systems, UHC and healthier populations.
VII. Prioritize the quality and performance of staff at each WHO level, and de-politicize recruitment (especially at senior levels) by adhering to criteria of merit and relevant competencies.
[p.52] 4. Establish a new international system for surveillance, validation and alert The Panel recommends I. WHO to establish a new global system for surveillance, based on full transparency by all parties, using state-of-the-art digital tools to connect information centres around the world and including animal and environmental health surveillance, with appropriate protections of people’s rights.
II. WHO to be given the explicit authority by the World Health Assembly to publish information about outbreaks with pandemic potential on an immediate basis, without requiring the prior approval of national governments.
III. WHO to be empowered by the World Health Assembly to investigate pathogens with pandemic potential in all countries with short-notice access to relevant sites, provision of samples and standing multientry visas for international epidemic experts to outbreak locations.
IV. Future declarations of a PHEIC by the WHO Director-General should be based on the precautionary principle where warranted, as in the case of respiratory infections. PHEIC declarations should be based on clear, objective, and published criteria. The Emergency Committee advising the WHO Director-General must be fully transparent in its membership and working methods. On the same day that a PHEIC is declared, WHO must provide countries with clear guidance on what action should to be taken and by whom to contain the health threat…
Although the late winter wave of COVID-19 in the United States seems to have crested, the emergence of variant strains and ongoing questions about immunity and vulnerability leave open the real possibility of additional waves later this year. Meanwhile, there is a growing humanitarian crisis befalling South Asia – in particular, the tragedy unfolding in India, where the health care system has essentially collapsed and many victims of COVID-19 are unable to receive any level of care whatsoever.
These current events should make clear how important it is to prepare for future waves of the virus, as the fight against COVID-19 is not over. We must promote vaccination at every turn, support efforts to share clinical and operational lessons learned in order to make improvements based on this past year’s experiences, and ready our health care system and communities for the potential for further surges in demand for care.
The prospect of once again facing decisions about whether to transition to crisis standards of care (CSC) calls for action now, while a relative lull in cases allows stakeholders to plan thoughtfully for such decisions. This is especially important in light of painful lessons the pandemic has taught about the need for clarity and consistency across institutions and jurisdictions about invoking CSC and the disproportionate impact COVID-19 has had on historically minoritized and marginalized populations. Going forward, addressing equity must be recognized as a vital consideration for refining and deploying CSC. The challenge of CSC that are not sensitive to issues of equity can be compounded when they are put into practice through processes that similarly fail to embed considerations of equity.
As a concept, CSC were originally designed to involve declarations from the state government when invoked. Unfortunately, in jurisdictions where these declarations occurred during the pandemic, CSC was not needed in many cases. On the other hand, in many jurisdictions where health care providers were making difficult triage decisions, there was no formal recognition of the application of CSC. Further, “declarations” were difficult because only certain aspects of the response qualified as CSC (e.g., the supply of personal protective equipment), while others were not. The actions of the state should be tied to the necessary actions of clinicians (e.g., liability protections for certain actions, statewide clinical guidance).
The role of the state increases as the clinical situation becomes dire. However, political considerations may preclude appropriate acknowledgement of challenging conditions. The expectations in each state should be clearly understood and agreed to by health care leaders and policy makers.
Going forward, the following actions would support a more efficient response: :: Ensuring that health care facilities in a given area have common indicators and agreed-on thresholds for what is considered “crisis” –in terms of both staffing and decisions being made. :: Creating messages for health care providers and the public to communicate effectively about what to expect from the health care system when crisis thresholds are reached. :: Ensuring that strategies are in place to “load-balance” patients and resources regionally to avoid triage decisions, particularly decisions that are likely to lead to adverse and inequitable outcomes. :: Briefing local officials on response plans and providing situational updates, thereby encouraging recognition of crisis situations “on the ground” as well as official support for the response.
Providers have significant concerns about their liability protections under CSC. Protections vary significantly by state. Although the “reasonable provider” standard does provide some overall protection, the following actions would provide greater clarity and security: :: Understanding what protections are provided by the state and federal laws. :: Ensuring that legal counsel in health care facilities/systems understands the importance of developing policy for CSC resource allocation decisions, rather than leaving decisions to providers. Legal counsel should be prepared to defend the system and provider decisions.
The concept of “triage teams” was designed to support decision making when the outcome of a decision may be grave (e.g., ventilator allocation). This construct proved too narrow due for the breadth and novelty of the decisions faced by providers during the COVID-19 pandemic, which were often ad hoc and difficult. Going forward, the following strategies would improve care and decision making: :: Ensuring that any provider facing a novel/uncomfortable allocation decision has a designated point of contact to obtain immediate expert advice (e.g., an intensivist on call) and a channel to raise the issue to an incident management team. :: Employing a standardized assessment of the goals of care with the patient and family at the time of hospitalization and reconsidering for the continuation of therapies when the patient’s condition changes. :: Ensuring the availability of palliative care providers to support providers as well as family and patient needs and to facilitate more complicated decision making; and encouraging best practices of palliative care to enhance the comfort of all patients and ensure that care is consistent with patient wishes. :: Developing facility/system policy to support common allocation decisions (e.g., strategies adopted house-wide to stretch dialysis or oxygen resources) whenever possible. :: Emphasizing that staff should not be taking upon themselves decisions to restrict resources (e.g., withholding mechanical ventilation due to personal interpretation of resource scarcity or impending scarcity).
Among the biggest challenges for health care systems throughout COVID-19 has been having too few staff with appropriate training to meet the needs of incoming patients, particularly for emergency and critical care. Going forward, the following actions would help ameliorate the effects of this shortage: :: Providing health care staff with support, respite, information about behavioral health resources, and monitoring/check-ins for adverse personal impacts. :: Assessing intent of staff in the next 6-12 months to retire, re-train, or cut back hours to avoid potential dramatic impact on staffing after COVID-19. :: Educating staff about plans during any future surge (e.g., plans for expanding space or staff, triggers, and expectations for how staff will be deployed). :: Ensuring that staff have access to education (proactive and just-in-time) as well as onboarding and mentoring for non-traditional positions. :: Developing regional plans for surge staffing that avoid direct competition among facilities and systems for contract and other staff, and ensuring that communities plan support needs for hospital staffing prior to the staffing of community-based alternate care sites.
Hospitals and health care providers have responded with great skill to the burdens of COVID-19. Whatever challenges lie ahead, a partnership between clinical and administrative staff, including legal counsel, is necessary in order to ensure the development of channels to share information and develop policies that will mitigate the consequences of resource shortages and moral distress that accompanies rationing decisions. Further, hospitals are not islands – connection between and across jurisdictions and regions is needed to load-balance patients and resources in the interest of fairness and equity – both key goals of CSC.
The best time to address these issues is now, while they are top of mind. Failure to capitalize on this opportunity means the continuation of a fractured system that could do much more to protect both patients and providers in times of crisis.
Reducing Global COVID Vaccine Shortages: New Research and Recommendations for US Leadership
Duke Margolis Center for Health Policy :: Mark McClellan, MD, PhD. Krishna Udayakumar, MD, MBA, Michael Merson, MD, Gary Edson, JD, MBA Policy Brief – April 15, 2021 :: 12 pages
PDF: https://healthpolicy.duke.edu/sites/default/files/2021-04/US%20Vaccine%20Access%20Leadership.pdf Abstract
A small number of high- and middle-income nations and regions including the United States (US), United Kingdom (UK), the European Union (EU), China, and India account for the majority of COVID-19 vaccines administered thus far. The uneven global distribution of COVID-19 vaccines has raised concerns and spurred demand for action to ensure equitable access, including growing calls to waive intellectual property protections. There are a number of challenges to scaling-up global access beyond intellectual property barriers, and addressing these challenges requires a multipronged, coordinated approach. Leadership from the US on safe, effective, and equitable global access to COVID-19 vaccines is imperative. In this paper, we present the scope of the global vaccine access challenge, and propose a complementary three-part US-led solution that: 1) increases and leverages funding for the global effort to advance vaccine access through COVAX; 2) undertakes coordinated bilateral and multilateral mechanisms to provide excess doses to countries in need; and 3) increases safe and reliable manufacturing and distribution capacity.
[Excerpts p.6-8]
…The following key principles should drive the strategy and priorities for access and distribution involving this robust manufacturing capacity:
:: Allocation and distribution should be equitable, based on the evolving burden from COVID-19 and urgency of need relative to available health resources;
:: Each country should have sufficient vaccine supply to protect its own population, while maximizing support for all other nations to do so to end the pandemic as quickly as possible; and
:: Timing is critical – countries with excess doses should release them to other countries provided that domestic needs are met, including “manufacturing slot swaps,” which achieves both adequate supply and accelerates availability to help save lives and protect health systems globally…
Vaccine allocation and distribution could occur through three potentially complementary mechanisms: (1) Donation through COVAX: As the global multilateral platform for COVID-19 vaccine access, COVAX could channel donated doses through its existing population-based allocation framework and infrastructure. COVAX partners have extensive experience deploying vaccines to low-income nations, working with UNICEF, providing one system for advancing equity across the world. However, this model and COVAX’s tripartite governance is untested at scale against a shifting and massive pandemic challenge. Moreover, in its first phase, COVAX is allocating doses primarily based on population. This could help avoid political biases in allocations, but could also result in vaccine allocation that is less effective in controlling the pandemic.
(2) Bilateral donations or loans (PEPFAR model): The US can lead by example through bilateral donations or loans to specific countries. A complementary strategy to COVAX would be to use a bilateral program, modeled on PEPFAR, that would include supplying not just the doses but also technical and managerial support and funding to assure supply and distribution logistics and training of health workers. For HIV and antiretroviral therapy, PEPFAR brought together the range of resources – including USAID, CDC, DoD, and the Peace Corps – to provide the coordinated support required to address local distribution challenges and uncertainty or hesitancy about treatment. Similar assistance now could build on PEPFAR experience and resources.
Factors for consideration in distributing excess vaccines to countries could include: disease burden, capacity of health systems, US ability to leverage existing distribution systems or provide added technical assistance (existing infrastructure, for example through PEPFAR and bilateral immunization programs, could help deliver vaccines and eventually antiviral treatments), and trade and diplomatic considerations (Mexico, Central and South America). The bilateral approach may be particularly important for efforts to distribute mRNA-based vaccines due to the current cold-chain storage and distribution requirements. In taking these steps, the US should encourage similar initiatives by other G7 countries that could be implemented in parallel to multi-lateral efforts, just as the US coupled PEPFAR with support for the multilateral Global Fund to Fight AIDS, Tuberculosis, and Malaria. Importantly, bilateral and multilateral efforts should be coordinated such that countries receive the same vaccine from different sources, augmenting distribution capabilities without fragmentation of support.
(3) Use of multi-lateral platforms independent of COVAX: This model would build upon recent announcements regarding the Quad platform to provide financing for additional vaccine manufacturing capacity in the Asia/Pacific region in partnership with India, Japan, and Australia. The US could provide donations of vaccines as well as financing and technical assistance through the Quad and other existing multilateral platforms, such as the African Union/Africa CDC joint COVID-19 African Vaccine Acquisition Task Force (AVATT), and the Africa Medical Supplies Platform (AMSP),and regional bodies such Association of Southeast Asian Nations (ASEAN).
With increasing vaccination and better outbreak control in the US and other high-income countries, the approach used here can facilitate timely redirection of manufacturing capacity to other countries, paving the way to faster global control….
COVID-19 Data Explorer: Global Humanitarian Operations COVID-19 Vaccine Roll-out
May 15, 2021 | COVAX (WHO,GAVI,CEPI), UNDESA, Press Reports | DATA Global COVID-19 Figures: 161M total confirmed cases; 3.3M total confirmed deaths Global vaccines administered: 1.40B
Number of Countries: 26
COVAX First Allocations (Number of Doses): 73M
COVAX Delivered (Number of Doses): 14M
Other Delivered (Number of Doses): 24M
Total Delivered (Number of Doses): 38M
Total Administered (Number of Doses): 20M
Weekly Epidemiological and Operational updates Last update: 15 May 2021 Confirmed cases :: 161 513 458 [week ago: 156 496 592] Confirmed deaths :: 3 352 109 [week ago: 3 264 143] Vaccine doses administered: No data at inquiry
::::::
Press conferences on COVID-19 14/05/2021 :: 54:01 WHO DG: “I understand why some countries want to vaccinate their children and adolescents, but right now I urge them to reconsider and to instead donate vaccines to COVAX”
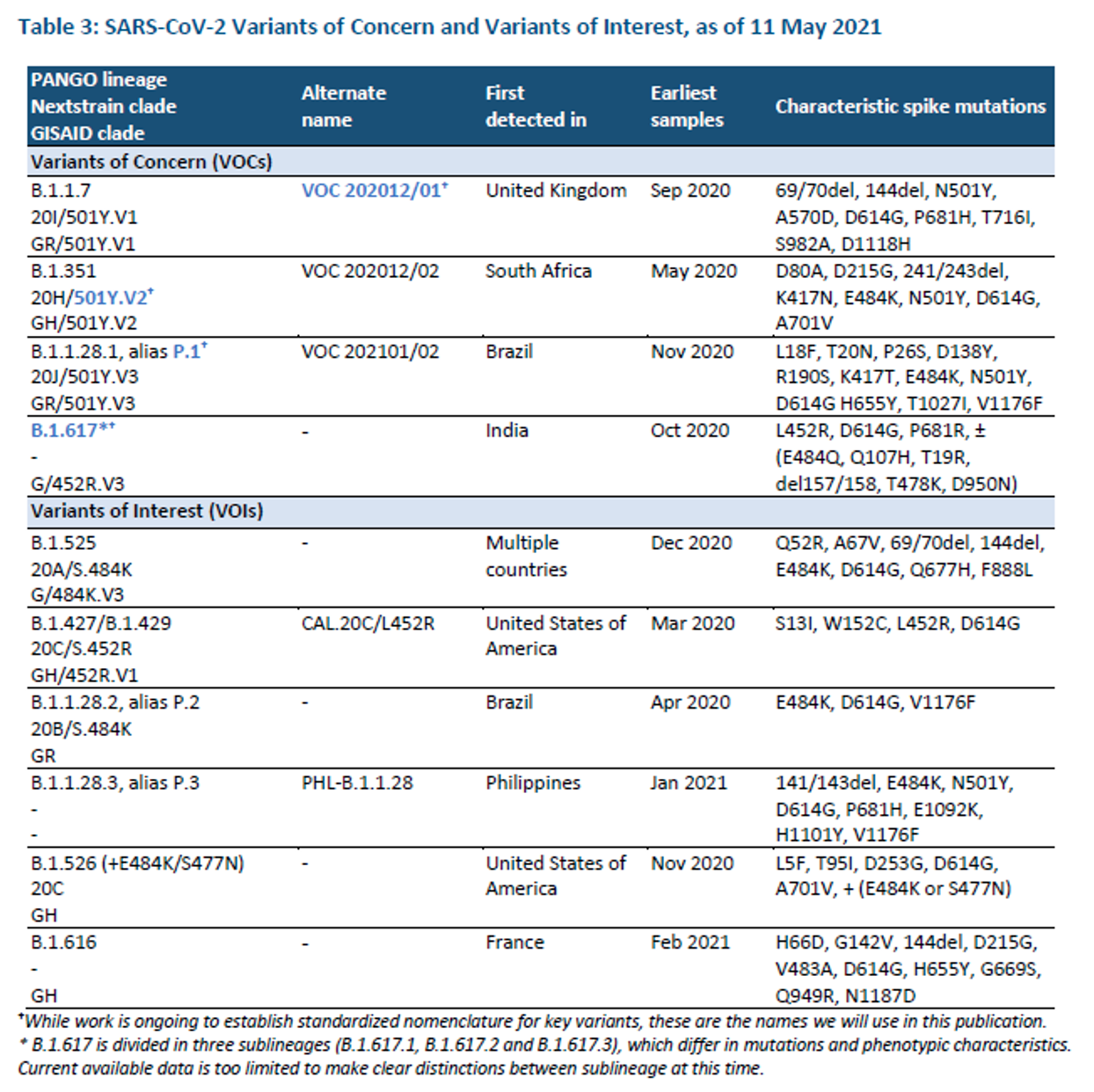
Weekly epidemiological update on COVID-19 – 11 May 2021 Overview Global overview: The number of new COVID-19 cases and deaths globally slightly decreased this week, with over 5.5 million cases and over 90 000 deaths. Case and death incidences, however, remain at the highest levels since the beginning of the pandemic. New weekly cases decreased in the regions of Europe and Eastern Mediterranean, while the South-East Asia Region continued an upward trajectory for 9 weeks and reported a further 6% increase last week. Special focus: In this edition, special focus updates are provided on four SARS-CoV-2 variants of concern [B.1.1.7 (VOC202012/01); B.1.351 (501Y.V2); P.1; B.1.617] and six variants of interest, including the geographic distribution, and phenotypic impacts on transmissibility, vaccines, therapeutics and diagnostics.
Weekly operational update on COVID-19 – 10 May 2021 Overview In this edition of the Weekly Operational Update on COVID-19, highlights of country-level actions and WHO support to Member States include: :: Equipment donated to support Belize’s COVID-19 vaccine deployment :: Strengthening International Health Regulations capacities at points of entry during COVID-19 in the Republic of Moldova :: Strengthening COVID-19 contact tracing efforts in the Philippines :: COVID-19 vaccination campaign in Bhutan: from planning to execution :: Rapid assessment of medical oxygen and biomedical equipment requirements in Guinea Bissau :: Launching of COVID-19 vaccination Intra-Action Reviews (IAR) :: Readiness for COVID-19 vaccination through simulation in Trinidad and Tobago :: Tips to celebrate Eid-El-Fitr safely, a position paper COVID-19 vaccination in humanitarian settings and multi-platform dissemination of WHO online courses in Portuguese :: Regular updates on WHO’s resource requirements and funds received to support countries in implementing the COVID-19 Strategic Preparedness and Response Plan 2021, WHO/PAHO procurement of critical supplies, and implementation of the Unity Studies
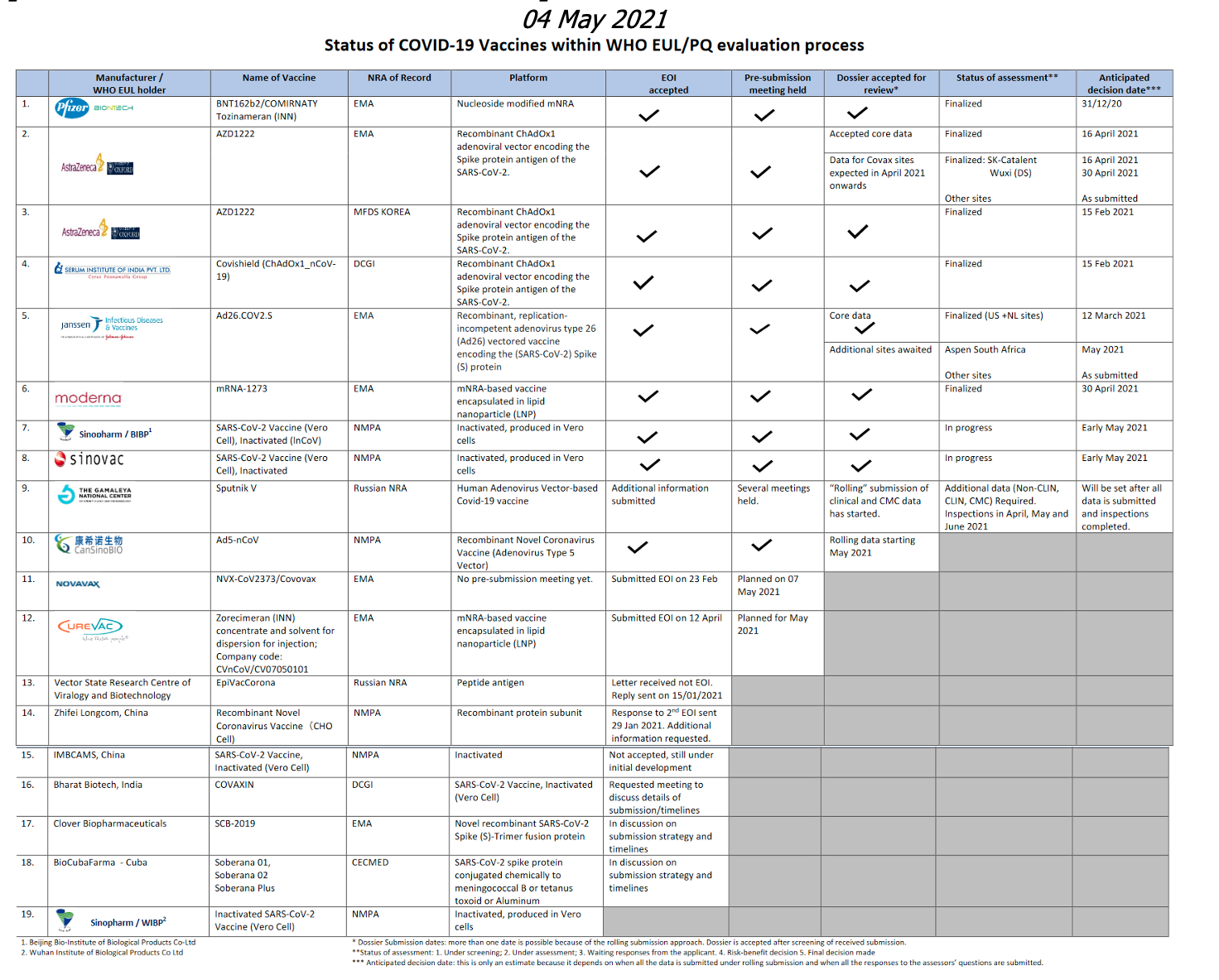
Status of COVID-19 Vaccines within WHO EUL/PQ evaluation process 23 April 2021 For 19 vaccine candidates, presents Manufacturer, Name of Vaccine, NRA of Record, Platform, EOI Accepted Status, Pre-submission Meeting Held Status, Dossier Accepted for Review, Status of Assessment; Anticipated/Completed Decision Date [click on the link above for full scale view]
COVID Vaccine Developer/Manufacturer Announcements [organizations from WHO EUL/PQ listing above]
AstraZeneca Press Releases– No new digest announcements identified
Bharat Biotech, India Press Releases – Website not responding at inquiry
BioCubaFarma – Cuba Últimas Noticias– No new digest announcements identified
CanSinoBIO News – No new digest announcements identified
Clover Biopharmaceuticals – China News – No new digest announcements identified
Curevac [Bayer Ag – Germany] News
May 13, 2021 Second-Generation COVID-19 Vaccine Candidate, CV2CoV, Demonstrates High Immunogenicity Against Virus Variants in Preclinical Study
May 13, 2021
:: Second-generation lead COVID-19 vaccine candidate, CV2CoV, developed in collaboration by CureVac and GSK
:: CV2CoV mRNA shows high levels of antigen production in rat model
:: Fast onset of strong neutralizing antibody titers after first vaccination
:: High cross-neutralizing capacity of induced antibodies against selected Variants of Concern
Gamaleya National Center Latest News and Events – No new digest announcements identified [See Russia/RFID below]
IMBCAMS, China Home – No new digest announcements identified
Janssen/JNJ Press Releases – No new digest announcements identified
Novavax Press Releases Novavax Statement on Updated PREVENT-19 Trial Protocol
Statement = COVID-19
5/10/2021
An updated protocol version 8.0 for our PREVENT-19 Phase 3 clinical trial (the PRE-fusion protein subunit Vaccine Efficacy Novavax Trial) was posted to the Novavax website today. PREVENT-19 is a randomized, observer-blinded, placebo-controlled study evaluating the efficacy, safety, and immunogenicity of NVX-CoV2373 with Matrix-M™ adjuvant in up to 30,000 subjects 18 years of age and older compared with placebo. The company’s pivotal Phase 3 study in the U.S. and Mexico began in December 2020 and significant progress has been made to-date, with final data expected in the second quarter of 2021…
EARLY RELEASE: The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine in Adolescents Aged 12-15 Years – United States, May 2021 Early Release / May 14, 2021 / 70 Summary What is already known about this topic? On May 10, 2021, the Food and Drug Administration expanded Emergency Use Authorization for the Pfizer-BioNTech COVID-19 vaccine to include adolescents aged 12–15 years. What is added by this report? On May 12, 2021, after a systematic review of all available data, the Advisory Committee on Immunization Practices made an interim recommendation for use of the Pfizer-BioNTech COVID-19 vaccine in adolescents aged 12–15 years for the prevention of COVID-19. What are the implications for public health practice? The Pfizer-BioNTech COVID-19 vaccine is the first COVID-19 vaccine approved for use in adolescents and has high efficacy against symptomatic COVID-19. Vaccination will be important to protect adolescents against symptomatic COVID-19 disease and to reduce community transmission of SARS-CoV-2.
“The FDA’s expansion of the emergency use authorization for the Pfizer-BioNTech COVID-19 Vaccine to include adolescents 12 through 15 years of age is a significant step in the fight against the COVID-19 pandemic,” said Acting FDA Commissioner Janet Woodcock, M.D. “Today’s action allows for a younger population to be protected from COVID-19, bringing us closer to returning to a sense of normalcy and to ending the pandemic. Parents and guardians can rest assured that the agency undertook a rigorous and thorough review of all available data, as we have with all of our COVID-19 vaccine emergency use authorizations.”…
Today, the U.S. Food and Drug Administration expanded the emergency use authorization (EUA) for the Pfizer-BioNTech COVID-19 Vaccine for the prevention of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) to include adolescents 12 through 15 years of age. The FDA amended the EUA originally issued on Dec. 11, 2020 for administration in individuals 16 years of age and older.
“The FDA’s expansion of the emergency use authorization for the Pfizer-BioNTech COVID-19 Vaccine to include adolescents 12 through 15 years of age is a significant step in the fight against the COVID-19 pandemic,” said Acting FDA Commissioner Janet Woodcock, M.D. “Today’s action allows for a younger population to be protected from COVID-19, bringing us closer to returning to a sense of normalcy and to ending the pandemic. Parents and guardians can rest assured that the agency undertook a rigorous and thorough review of all available data, as we have with all of our COVID-19 vaccine emergency use authorizations.”…
European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en Latest Updates Threat Assessment Brief: Emergence of SARS-CoV-2 B.1.617 variants in India and situation in the EU/EEA
11 May 2021 Executive summary
:: First reported in India in December 2020, SARS-CoV-2 lineages B.1.617.1, B.1.617.2 and B.1.617.3 have been increasingly detected in other countries.
:: The aim of this Threat Assessment Brief is to assess the potential public health implications of the B.1.617 lineages for EU/EEA countries with a focus on lineage B.1.617.2.
:: Over the past eight weeks India and some surrounding countries have seen a sharp increase in the number of reported SARS-CoV-2 cases and deaths. This has been associated with a rising proportion of sequenced viruses belonging to lineages B.1.617.1 and B.1.617.2.
:: The United Kingdom has seen a rapid increase in detection of lineage B.1.617.1 and, to a greater extent, B.1.617.2, associated with travel to India and onward community transmission. On the 6 May, the United Kingdom (UK) designated lineage B.1.617.2 as a variant of concern.
:: In the EU/EEA there are indications that the frequency of detection of both lineages B.1.617.1 and B.1.617.2 is increasing.
:: Currently described lineages B.1.617.1, B.1.617.2 and B.1.617.3 have distinct mutation profiles and warrant individual assessment. Given the still very limited available data with respect to their transmissibility, disease severity and immune escape potential relative to other co-circulating SARS-CoV-2 variants in the EU/EEA, the full impact of these lineages on public health is not yet possible to assess.
:: At this time, ECDC maintains its assessment of B.1.617.1, B.1.617.2 and B.1.617.3 as variants of interest and will continue to actively monitor the situation.
Press release 11 May 2021 Sahel and Central Africa: €210 million in EU humanitarian aid
The EU is reaffirming its solidarity with vulnerable people in countries in the Sahel and Central Africa through a humanitarian budget of €210 million in 2021.
Vaccination with Sputnik V launched in India
Press release, 14.05.2021
…Sputnik V has become the first foreign-made vaccine that is used in India contributing to the world’s largest COVID-19 vaccination campaign.
Inoculations with Sputnik V in Hyderabad today followed the arrival of the first batch of the vaccine in India on May 1, 2021. The second batch of Sputnik V is expected to arrive in India by the end of the week.
Sputnik V was approved for use in India on April 12, 2021 and granted an emergency use authorization. India is the leading production hub for Sputnik V. RDIF has reached agreements with the leading pharmaceutical companies in the country (Gland Pharma, Hetero Biopharma, Panacea Biotec, Stelis Biopharma, Virchow Biotech) aimed at production of more than 850 million doses per year…
Government of India – Press Information Bureau Latest Press Releases PM chairs a high level meeting on Covid and vaccination related situation Posted on: 15 May 2021 PM chaired a high-level meeting to discuss the Covid and vaccination related situation in the country. Officials briefed the PM on the current Covid related situation in the country…. …PM said that India’s fight against Covid has been guided throughout by scientists and subject experts and will continue being guided by them. Officials briefed PM about the vaccination process and the state-wise coverage of 45+ population. The roadmap for future vaccine availability was also discussed. He directed officials to work closely with states to ramp up the speed of vaccination.
POLIO Public Health Emergency of International Concern (PHEIC)
Polio this week as of12 May 2021
:: The GPEI has released the 2021 National Emergency Action Plan (NEAP) for Afghanistan which contains the current epidemiology and situational overview and progress on the 2020 NEAP among other contents.
:: The latest issue of the newSpecial magazine features an article titled “Experience in eradicating polio helps COVID-19 response” which details the role that polio workers have played in fighting the pandemic. The article is available here on page 34.
:: Last week, the GPEI and UN Foundation together with the UK and UAE Missions to the UN in New York hosted a high-level dialogue looking at the intersection of gender and immunization. The panelists made recommendations on championing women & girls in immunization, drawing on the polio programme. Watch the recorded discussion here.
Summary of new WPV and cVDPV viruses this week (AFP cases and ES positives):
:: Afghanistan: two cVDPV2 positive environmental samples
:: Benin: one cVDPV2 case
:: Burkina Faso: one cVDPV2 case
:: Liberia: one cVDPV2 case
:: Sierra Leone: two cVDPV2 positive environmental samples
:: Tajikistan: two cVDPV2 positive environmental samples
:: Yemen : one cVDPV1 case
:::::: ::::::
WHO/OCHA Emergencies
Editor’s Note:
Continuing with this edition, we include information about the last apparent update evident on the WHO emergency country webpages, recognizing almost universal and significant interims since last update regardless of the level of the emergency listed.
Democratic Republic of the Congo– No new digest announcements identified [Last apparent update: 3 May 2021] Mozambique floods– No new digest announcements identified [Last apparent update: 3 November 2020] Nigeria– No new digest announcements identified [Last apparent update: 29 Jun 2020] Somalia– No new digest announcements identified [Last apparent update: 17 July 2020] South Sudan– No new digest announcements identified [Last apparent update: 4 February 2020] Syrian Arab Republic– No new digest announcements identified [Last apparent update: 24 October 2020] Yemen– No new digest announcements identified [Last apparent update: 30 June 2020]
Iraq–
:: Iraq receives second delivery of COVID-19 vaccines through the COVAX Facility
Baghdad, 12 May 2021 – Despite a continued global shortage and limited production of COVID-19 vaccines, on 9 May Iraq received the second shipment of the AstraZeneca COVID-19 vaccine through the COVAX Facility. The arrival of the second shipment of exactly 499 200 doses brings the total number of vaccines received by the Iraqi health authorities from the COVAX Facility to nearly one million….
Afghanistan– No new digest announcements identified [Last apparent update: 5 July 2020] Angola– No new digest announcements identified [Last apparent update: 16 March 2021] Burundi– No new digest announcements identified [Last apparent update: 04 July 2019] Cameroon– No new digest announcements identified [Last apparent update: 22 August 2019] Central African Republic– No new digest announcements identified [Last apparent update: 12 June 2018] Ethiopia– No new digest announcements identified [Last apparent update: 22 August 2019] Iran floods 2019– No new digest announcements identified [Last apparent update: 2 March 2020] Libya– No new digest announcements identified [Last apparent update: 7 October 2019] Malawi– No new digest announcements identified [Last apparent update: 22 April 2021 Measles in Europe– No new digest announcements identified [Last apparent update: 26-04-2021] MERS-CoV– No new digest announcements identified [Last apparent update: 8 July 2019] Mozambique– No new digest announcements identified [Last apparent update: 03 November 2020] Myanmar– No new digest announcements identified [Last apparent update: 29 March 2021] Niger – No new digest announcements identified [Last apparent update: 16 avril 2021] occupied Palestinian territory– No new digest announcements identified [Last apparent update: 4 September 2019] HIV in Pakistan– No new digest announcements identified [Last apparent update: 27 August 2019] Sao Tome and Principe Necrotizing Cellulitis (2017)– No new digest announcements Sudan– No new digest announcements identified [Last apparent update: 24 June 2020] Ukraine– No new digest announcements identified [Last apparent update: 1 May 2019] Zimbabwe– No new digest announcements identified [Last apparent update: 10 May 2019]
Chad– No new digest announcements identified [Last apparent update: 30 June 2018] Djibouti– No new digest announcements identified [Last apparent update: 25 novembre 2020] Kenya– No new digest announcements identified [Last apparent update: 23 April 2021 Mali– No new digest announcements identified [Last apparent update: 3 May 2017] Namibia – viral hepatitis – No new digest announcements identified [Last apparent update: 20 July 2018] Tanzania– No new digest announcements identified [Last apparent update: 21 October 2019]
WHO Regional Offices Selected Press Releases, Announcements WHO African Region AFRO
:: What fuels the use of unproven COVID-19 therapies? 14 May 2021
The emergence of COVID-19 and the pandemic have raised many challenges regarding treatment and spawned the use of unproven therapies. Professor Lucille Blumberg, the Deputy Director of the South African National Institute for Communicable Diseases, discusses the causes, the risks and how to tackle unproven COVID-19 cures.
:: Risks and challenges in Africa’s COVID-19 vaccine rollout 14 May 2021
Africa’s largest-ever vaccination drive is well under way. Forty-nine African countries are rolling out COVID-19 vaccines and over 22 million doses have been given on the continent. Valuable lessons are emerging, but major risks and challenges threaten Africa’s fragile gains.
:: Joining forces to tackle the Ebola Infodemic in Guinea 12 May 2021
On a sultry morning in early March in the small town of Gouécké in south-eastern Guinea, scores of concerned community and customary leaders gathered for a meeting with WHO’s local team of social anthropologists.